Review of the Peabody Developmental Motor Scales Assessment
Introduction [edit | edit source]

The Peabody Developmental Motor Calibration was first developed and published in 1983 by Rhonda Page and Rebecca Fewell.[1] A second edition was published in 2000 by the same authors (PDMS-2).[2]
No specific course or accreditation is needed to exist able to conduct the examination, merely it is valuable to take good knowledge of the developmental stages of a child. A wide variety of healthcare professionals, such equally physiotherapists, occupational therapists, psychologists, doctors and physical education teachers, can perform the test in the assessment of a child with possible developmental delay or issues. A proficient noesis base in normal and typical evolution also equally in singular development is recommended. This will get in easier to understand the nuances in the development of children.[3] The assessment kit is available for buy online.
Benefits of the PDMS-ii [edit | edit source]
- Splendid tool for the evaluation of the motor evolution of young children past providing separate tests and grading scales for both gross motor skills and fine motor skills[iv]
- Exam battery standardisation carried out with a full of 2003 children in the USA and Canada and is the first bombardment that was standardised on a national level[two] [4]
- The only tool of its kind that combines evaluation with the planned intervention. A planned plan of 104 motor teaching and therapy activities is included.[two] [4]
- These activities are organised based on the child's development. The programme can help in:
- The development of skills provided that the evaluation of a child'due south skills based on the test battery has been completed.[4]
Application of the PDMS-2 [edit | edit source]
The test was designed to identify developmental delays in children. The test can be used in various populations and settings to reach specific goals. These may include[2] [iii]:
- Assessing a kid's motor competence relative to his/her peers
- For case in a clinical setting where children with diverse diagnosis and a wide range of neuromuscular impairments tin can be assessed and therapy provided
- Identifying delays or disorders in the development
- For example in a school setting – i.east. At a preschool, to selection up on children that may have a developmental delay also as their strengths and weaknesses
- A useful tool to evaluate a kid's progress
- The test was developed to identify strengths and weaknesses in a kid'south motor development. Administering the exam before and after a physical therapy intervention plan is a good manner to document the child'due south progress and to measure the efficacy of the intervention.
- Inquiry purposes
- PMDS-2 is the gold standard and is often used in research and literature to assess the nature of motor development in various populations of children
- Specific skill deficits can be used to develop individualised goals.
- Helps in designing treatment goals and treatment plan based on the child's strengths and weaknesses in motor development
Administrator Qualification [edit | edit source]
No specific class or accreditation is needed to exist able to behave the test, but it is valuable to have good noesis of the developmental stages of a child. A wide variety of healthcare professionals can perform the examination in the assessment of a child with possible developmental delay or issues. These may include:
- physiotherapists
- occupational therapists
- psychologists
- doctors
- physical education teachers
A good knowledge base in normal and typical development likewise as in singular evolution is recommended. This will make it easier to understand the nuances in the evolution of children.[three] It is also recommended to have a thorough agreement of[five]:
- exam statistics
- the general procedure governing exam administration
- scoring and interpretation of the score
- specific information nigh gross and fine motor skills testing
- development in children who are non progressing typically to their peers
Validity and Reliability of PDMS-2 [edit | edit source]
The PDMS-two has been proven as a reliable and valid measurement tool in various paediatric populations, such as:
- Children on the autistic spectrum[six]
- Children with cerebral palsy[seven]
- Premature children and babies[8] [nine]
- Children receiving concrete therapy for various diagnoses[10] [11]
Target Population [edit | edit source]
The Peabody Developmental Motor Scale -2 is advisable and should be used for children from nascence to 5 years (72 months) old.[ii]
PDMS-ii Toolkit [edit | edit source]
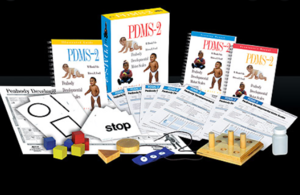
The Peabody Developmental Motor Scale -2 Toolkit is available for online purchase and consists of the following materials that are required to administer the test:
- Examiners manual
- includes the history of test development
- describes the validity and reliability measures of the test
- contains the various scoring charts
- The Guide to Item Assistants
- includes a clarification and images of each of the activities or skills assessed
- Motor Activities Program Book
- includes various ways/options in which to teach a child the skills that he/she is having difficulty with
- the importance of various skills is also discussed and highlighted
- Profile/Summary form
- certificate where all raw data can be added to create a scoring graph
- Examiners Record Booklet
- used by the therapist when administering the exam to score all activities or skills assessed
- Test Manipulatives document
- indicates what items are needed to administrate the examination, for instance, an 8-inch ball, tennis brawl, string, chair, tape measure, etc.
- Peabody Motor Development Chart
Administration of PDMS-ii [edit | edit source]
[edit | edit source]
- Read the transmission beforehand
- Accept someone help who is familiar with the test
- Run the test three times before actually concluding a score
- Calm and prissy surroundings
- Be sensitive to the child's limitations – avert the child condign frustrated[2]
Important Tips [edit | edit source]
- All assessment items should be presented in a precise manner with specific exact cues and demonstrations
- Administer test in an surround with minimal distractions
- The surface area where the exam is administered should be ready-upward beforehand, areas marked out and pre-measured and equipment ready. This is to avoid whatsoever disruptions during the test and allow the test to flow. Examples of areas to pre-measure out include[3]:
- A line on the floor clearly marked (spray paint or duct record) – 4 inches wide and 8 feet long
- An area where the child needs to run also marked out – 10 feet (3m) 30 feet (9m), 45 feet (13m) or converted to the metric system
- Jumping distances demarcated
- Jumping from dissimilar heights – take benches already ready and at correct heights
Description of the PDMS-2 [edit | edit source]

The Peabody Developmental Motor Scale (PDMS-2) assesses fine and gross motor skills of children from birth to 6 years old relative to their peers. There are 4 subtests well-nigh gross motor skills and two subtests almost fine motor skills. The gross motor subtests include[12]:
- Reflexes (birth to xi months)
- Stationary performances (all ages)
- Locomotion (all ages)
- Object manipulation (12 months and older)
The fine motor skills subtests include:
- Grasping (all ages)
- Visual-motor integration (all ages)
The total score is adamant by the sum of the points of each subscale/item. Every particular is rated on a 3-point rating scale. Internal consistency of the scale is very high (alpha = 0.97).[thirteen]
Fine Motor Skills Subtests [edit | edit source]
The items per subtest for the fine motor skills part of the PDMS-two are[ii]:
- Grasping
- Grasping cubes
- Grasping marking
- Buttoning/unbuttoning buttons
- Touching fingers
- Visual-motor integration
- Building belfry/train/bridge/wall/steps/pyramid
- Snipping with pair of scissors imitating horizontal stroke
- Stringing beads
- Folding paper
- Copying circumvolve/cross/square
- Cutting paper/line/circumvolve/square
- Lacing string
- Dropping pellets
- Tracing line
- Connecting dots
- Colouring betwixt lines
Administering the Gross Motor Role Part of the PDMS-ii [edit | edit source]
Often in multidisciplinary team set-ups, the physiotherapist will assess the gross motor part part and an occupational therapist will focus on the fine motor section. As already mentioned the complete PDMS-2 has 6 subtests. The get-go four focuses on gross motor skills and the concluding two on fine motor skills. For the purpose of this folio, the focus will be on the gross motor skill subtests.
Reflexes: [edit | edit source]
- This investigates the child's reaction to outside stimuli or the child's ability to automatically react to environmental events.
- This examination is but administered to children under the historic period of 1 year, as reflexes are typically integrated by the time a child is 12 months old.
- Eight different items are assessed nether reflexes. Some of these are:
- Walking reflex
[18]
-
- Positioning Reflex: Asymmetrical Tonic Cervix Reflex (integrated)
- Landau Reaction
[xix]
-
- Protecting Reaction - Forward
- Protection Reaction - Side
- Correct Reaction - Forward
- Protecting Reaction - Backward
Stationary [edit | edit source]
- This subtest assesses a child's ability to sustain control of his/her body within its centre of gravity and the ability to retain equilibrium

- Thirty different items are assessed nether Stationary. These tin can include:
- rotating caput
- stabilising torso
- sitting
- raising to sit
- standing on 1 leg
- continuing on toes
- initiation of movements such every bit:
- sit-ups
- push-ups
[20]
Locomotion [edit | edit source]
- This measures a child's ability to move from ane place to another

- This is the largest section of the PDMS-2 and assesses 89 items in this subtest. Actions that are measured include:
- crawling
- walking
- running
- hopping
- jumping forrad

- bearing weight
- rolling
- pushing upwardly
- moving forwards
- creeping
- scooting
- pivoting
- stairs climbing
- walking line
- jumping hurdles
- skipping
Object Manipulation [edit | edit source]
- This subtest measures a kid'south ability to manipulate balls, such as catching, throwing and kicking

- These skills are not credible until a kid is eleven months old, therefore this subtest is only administered in children ages 12 months and older
- This subtest includes 24 items. These include:
- catching a ball
- throwing a ball (overhand and underhand)
- kicking a brawl
- hitting target (overhand and underhand)
- bouncing a ball
- catching a bounced brawl
[edit | edit source]
In addition, the therapist is encouraged to observe and tape the following behaviours[v]:
- the child'southward interest in the task
- the child's arroyo to understanding the instructions
- the child'south approach to problem-solving
- the child's comments or not-verbal response to the chore
- the child's latency of response
- the child'southward use of self-corrections
- the kid's preferred paw used in throwing, grasping, etc
- the child's directionality in transferring materials
Grading and Scoring of the PDMS-ii [edit | edit source]
The therapist will inquire the child to practise a specific item and observes how the child is doing the task. Items are scored as 2, 1 or 0.
- 0 = child cannot or volition not attempt an particular or the attempt does not indicate that the specific skill is emerging
- ane = child's performance shows a articulate resemblance to item mastery criteria but does not fully meet the criteria or at that place are signs of an emerging skill
- 2 = child performs item according to the criteria specified for mastering the skill
It volition be as well time-consuming to administer the consummate the examiner's booklet for every child, and then it is recommended to begin or enter the exam at the entry point appropriate for the historic period of the child as marked in the scoring sheet. In the examiner's booklet, the different ages are marked in nighttime blue and this is where the exam is "entered" and continued from. The test will begin at the basal level. This is the level where a child receives a score of 2 on iii items in a row. The test will be stopped at the ceiling level. This is the level where a child scores 0 on each of three items in a row. This will exist done for each subtest.[two]
[21]
Note that the skills to exist assessed are all in chronological society. Therefore, if a child is not continuing still, the assessment will focus on activities such as rolling or itch, for example.[iii]
The duration of the examination is normally around 45 - hour. Some therapists adopt to do the gross motor and fine motor sections on different days, every bit doing them back to dorsum may be too much for the child.
At any point of the PDMS-two, 3 gross motor subsets volition be assessed. If the child is younger than 11 months, the three subsets included will be reflexes, stationary and locomotion. If the child is over 1 yr, the 3 subsets to be assessed volition be stationary, locomotion and object manipulation.
Examples of Scoring Subtest Items [edit | edit source]
Reflexes [edit | edit source]
When assessing the walking or stepping reflex in a child younger than 11 months, the therapist holds the child from nether his breast up on a table. Allow the child to have some automatic steps. If the kid is able to lift i pes and then the other in frontwards walking within three seconds, a score of 2 can be documented. If the child lifts one foot, merely cannot have the steps within three seconds, a score of ane can be documented. If the child'due south legs remain still and no steps are taken, a score of 0 can exist documented.[3]
Locomotion [edit | edit source]
The child is asked to walk on a line, iv inches wide and eight anxiety long. If the kid is able to walk on the line for six anxiety, a score of ii is allocated.[3]
Scoring of the PDMS-2 [edit | edit source]
Scoring of the PDMS-two is documented on the scoring profile or summary grade. This is done afterwards the administration of the exam. The raw data scores are used in conjunction with the various appendices bachelor in the PDMS-ii reference guide and the following standardised scores tin can be calculated from these[two]:
- Age equivalents
- Percentiles
- Standard scores
- Gross Motor Quotients
Raw Score [edit | edit source]
The raw score is the sum of the various scores (0,1 and two) on each of the items. As the test is "entered" at the basal level (where child scores three 2's in a row), it may exist causeless (and this assumption is congenital into the test) that the kid also scored ii's on all the items before the first (basal level) of the test. These items also needed to be added as part of the raw score.
Profile Summary [edit | edit source]
The raw data scores are added to the profile summary class. Information technology is key to know the child'south age before commencing with the assessment, and with prematurely born children, the corrected age will be used up until two years sometime.
In the examiner's manual, Table A is used to determine the child'southward percentile rank for the various subtests, based on the raw score accomplished. This percentile score can exist used every bit an indication of whether concrete therapy is needed. The standard score of the diverse subtests is also extracted from Table A and also added to the profile summary certificate.
Table B in the examiner'south manual will provide the gross motor score. The gross motor score is the sum of the standard scores of each of the subtests. Based on the gross motor score the percentile rank of the child's gross motor abilities is adamant.
Table C in the examiner'southward manual provides the age proficiency of the child for each of the divide subtests such every bit reflexes, stationary, locomotion and object manipulation.
On the Profile summary page, a graph can so exist drawn up, based on all the various scores obtained from Tables A, B and C in the examiner'south transmission.
[24]
Score Interpretation [edit | edit source]
It is important to consider that children from different countries may score differently from the scores provided in the PDMS-ii. For example, in Bharat, it has been shown that the children's gross motor skill norms are lower than in America.[25] Or in State of israel, where baseball is non really played, throwing a tennis ball overhand and underhand might be a bit more difficult for children. Cultural differences may play a part in administering the test and the choice of objects used.
In premature babies, the gross motor deficit may become stronger over time.[8] For instance, at 18 months, at that place may not exist much of a deficit, and the child'south score may fall within the wide developmental norm. Still, at the age of 5, the deficits may be more obvious. Therapists are recommended to consider this in their assessment and treatment of the child and re-evaluate on a regular ground to ensure that the gross motor skill evolution gap is not getting larger, but just getting smaller.
Therapy goals and planning [edit | edit source]
The Motor Activities Programme Volume is a very useful tool to consult in the planning of therapy and goal setting. It provides reasons for the child beingness able to perform the various skills. It also provides useful ways to accost developmental delays of each of the items and shows different examples of how to progress. It can provide the therapist with good ideas on how to start off with therapy and accost the specific developmental problems and also assist with the planning of a home program where parents or guardians can besides exist involved in helping the child.[iii]
Ultimately our goal of therapy is to exist able to help the child with developmental delays to exist a happier, productive, motor proficient and moving kid in his/her environment.[3]
References [edit | edit source]
- ↑ Page MR, Fewell RR. Peabody developmental motor scales and activity cards. DLM Teaching Resources; 1983.
- ↑ 2.0 2.1 two.2 ii.iii 2.four 2.5 two.6 2.vii 2.8 Folio MR, Fewell RR. PDMS-2 Peabody developmental motor scales 2nd edition. Austin: PRO-ED Inc. 2000.
- ↑ three.0 3.ane iii.two 3.3 iii.iv iii.five three.half dozen 3.seven 3.8 Taragin, A. Administration and Scoring of the Peabody Developmental Motor Scale - two. Course, Physioplus 2020.
- ↑ 4.0 4.one 4.ii 4.3 Dourou E, Komessariou A, Riga V, Lavidas One thousand. Cess of gross and fine motor skills in preschool children using the Peabody Developmental Motor Scales Musical instrument. Eur Psychomotricity J. 2017;ix:89-113.
- ↑ v.0 5.1 Peabody Developmental Motor Scales (PDMS)– 2 Erin Chang, OTS, Karinette Leano, OTS, Thanh Luong, OTS, and Lisa Mireles, OTS. Presentation on Slideshare. Available from https://www.slideshare.net/stanbridge/peabody-developmental-motor-scales-pdms-2 (last accessed 27 Baronial 2020).
- ↑ Holloway JM, Long TM, Biasini F. Relationships between gross motor skills and social function in young boys with an autism spectrum disorder. Pediatric physical therapy: the official publication of the Section on Pediatrics of the American Concrete Therapy Clan. 2018 Jul;thirty(three):184.
- ↑ Clutterbuck GL, Auld ML, Johnston LM. Loftier‐level motor skills assessment for ambulant children with cerebral palsy: a systematic review and decision tree. Developmental Medicine & Child Neurology. 2020 Jun;62(6):693-9.
- ↑ 8.0 8.i Tavasoli A, Azimi P, Montazari A. Reliability and validity of the Peabody Developmental Motor Scales-for assessing motor development of depression birth weight preterm infants. Pediatric neurology. 2014 Oct 1;51(4):522-6.
- ↑ Wang M, Mei H, Liu C, Zhang Y, Huixian LI, Yan F. Application of the Peabody developmental motor scale in the assessment of neurodevelopmental disorders in premature infants. Chinese Pediatric Emergency Medicine. 2017 January 1;24(10):760-three.
- ↑ Phillips D. Concurrent Validity and Responsiveness of the Peabody Developmental Motor Scales-2 (PDMS-2) in Infants and Children with Pompe Disease undergoing Enzyme Replacement Therapy.
- ↑ Parmar Sanjay KS. Applicability of Peabody developmental Motor Scales PDMS-2 as a developmental assessment scale for Indian children. Occup Ther Int. 2008;2:one-3.
- ↑ Karimi H, Aliabadi F, Hosseini Jam M, Afsharkhas L. Evaluation of motor skills in high-risk infants based on Peabody Developmental Motor Scales (PDMS-2). International Journal of Children and Adolescents. 2016 Jan 10;2(1):4-7.
- ↑ Minoliti R, Crepaldi M, Antonietti A. Identifying Developmental Motor Difficulties: A Review of Tests to Assess Motor Coordination in Children. Journal of Functional Morphology and Kinesiology. 2020 Mar;5(1):16.
- ↑ Mary Gavacs. MNE OTA 59 mo. # 7. Available from https://world wide web.youtube.com/watch?v=HS6cdiNozmE (last accessed 17 November 2020)
- ↑ Mary Gavacs. MNE OTA Peabody Developmental Motor Scales: Fine Motor Subtest, 48 mo, #8.(last accessed 17 November 2020)
- ↑ Mary Gavacs. MNE OTA PDMS 59 months #10. (last accessed 17 November 2020
- ↑ Mary Gavacs. MNE OTA PDMS 59 mo #9. (final accessed 17 November 2020)
- ↑ Nicole Edmonds. Spontaneous Stepping Reflex. Published on 22 October 2018. Available from https://world wide web.youtube.com/lookout man?v=cn7XPS21avE (last accessed thirty Baronial 2020)
- ↑ Salubrious Life. Postural Reflexes - Landau. Newborn Reactions (half-dozen months). Published on sixteen Nov 2014. Avaialable from https://world wide web.youtube.com/sentry?v=Q5pZNd93qEw. (last accessed 30 August 2020)
- ↑ Kaitlyn Morley. Stationary subset of PDMS-2. Published on 3 June 2015. Available from https://world wide web.youtube.com/spotter?five=rlo0gKpQ-ig&t=8s. (last accessed thirty August 2020)
- ↑ RP. Peabody Motor Skills Basal and Ceiling EXPLAINED!!!! Available from https://www.youtube.com/lookout man?v=XCrz-JwtRts. (last accessed 17 Nov 2020)
- ↑ Robby Carson. PDMS-two Scoring. Available from https://world wide web.youtube.com/watch?v=H6I0mxriCAU. (last accessed 17 November 2020)
- ↑ Robby Carson. Calculation and Interpretation of Scores of the Peabody. Available from https://www.youtube.com/watch?five=9iO5MqHKgxo&t=11s. (concluding accessed 17 November 2020)
- ↑ Cheyann Walters. Peabody Developmental Motor Scales - 2nd Edition. Published on sixteen September 2019. Available from https://www.youtube.com/watch?five=cVW1NrFrs08. (last accessed xxx August 2020)
- ↑ Tripathi R, Joshua AM, Kotian MS, Tedla JS. Normal motor development of Indian children on Peabody developmental motor scales-2 (PDMS-2). Pediatric Physical Therapy. 2008 Jul 1;xx(2):167-72.
Source: https://www.physio-pedia.com/Peabody_Developmental_Motor_Scale_%28PDMS-2%29
0 Response to "Review of the Peabody Developmental Motor Scales Assessment"
Post a Comment